David Guggisberg, MD; Smaı¨l Hadj-Rabia, MD; Caroline Viney, MD; Christine Bodemer, MD, PhD;Francis Brunelle, MD; Michel Zerah, MD, PhD; Alain Pierre-Kahn, MD; Yves de Prost, MD; Dominique Hamel-Teillac, MDSkin Markers of Occult Spinal Dysraphism in Children. A Review of 54 Cases. Arch Dermatol. 2004;140:1109-1115
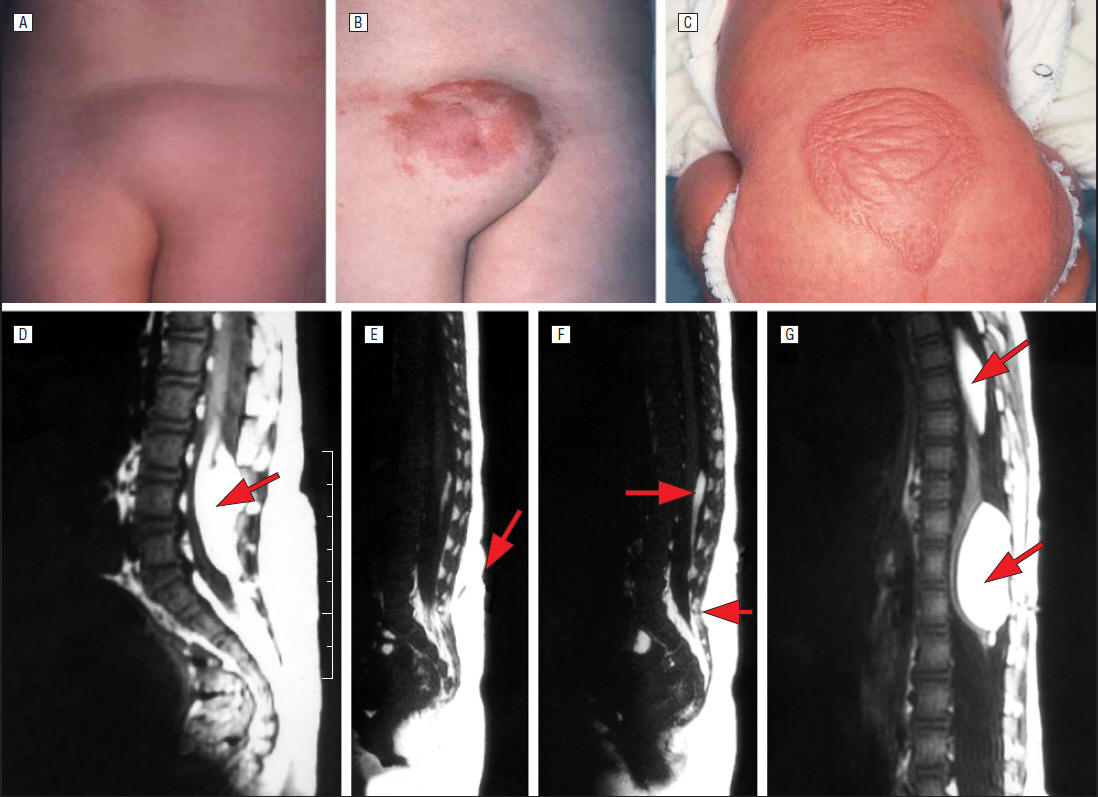
spinal cord (D-G). A, Sacral lipoma and deviated gluteal furrow (DGF); B, lumbar port-wine stain, lipoma, dermal sinus, and DGF; and C, dorsal and lumbar
unclassified hamartomas. D, Lipoma of the conus (arrow); E, dermal sinus (arrow); F, top of the lipoma of the filum terminale (upper arrow) and fistula (lower
arrow); G, multiple lipomas of the thoracic cord (upper arrow) and posterior conus (lower arrow).

Clinical aspects of isolated or combined congenital
median lumbosacral cutaneous lesions. A, Ulcerated hemangioma centered
on a dermal sinus and
deviation of the gluteal furrow; B, isolated port-wine stain; C, human
tail; D, faun tail.
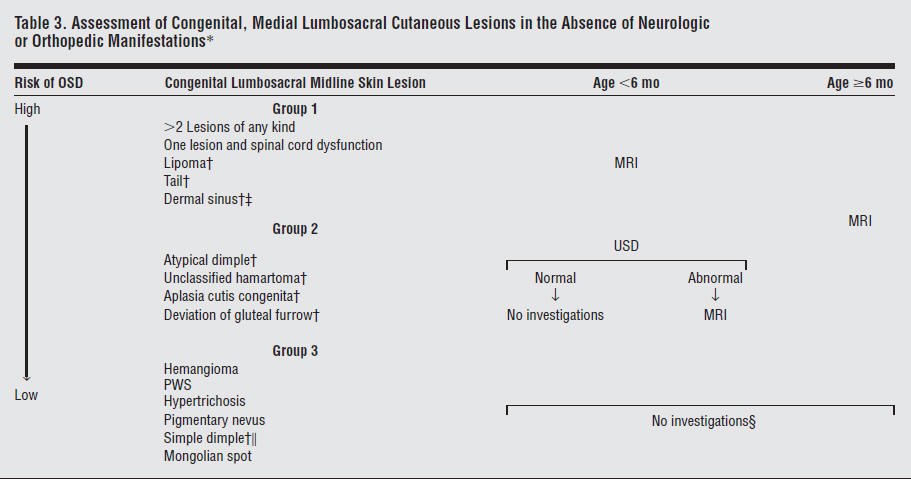 Abbreviations: MRI, magnetic
resonance imaging; OSD, occult spinal dysraphism; PWS, port-wine stain;
USD, ultrasound.
Abbreviations: MRI, magnetic
resonance imaging; OSD, occult spinal dysraphism; PWS, port-wine stain;
USD, ultrasound.*Neurologic and morphologic evaluations are required in the presence of clinical symptoms.
†Considered as isolated lesion.
‡High risk of cerebrospinal fluid infection leading to rapid spinal MRI and neurosurgical evaluation.
§All authors do not agree with this opinion for isolated PWS.
Simple dimple is defined as an isolated small lesion ( 5 mm in diameter) 2.5 cm or closer to the anus.